In-Hospital Quality Outcomes for Hepatocellular Carcinoma with Gastrointestinal Hemorrhage
In Hepatocellular Carcinoma (HCC)
Get Dexur’s Personalized Hospital Specific Presentation on Quality, Safety, Compliance & Education
By: James Pitt Dec. 19, 2018
2013-2017 Update on GI Hemorrhage in Hepatocellular Carcinoma
Gastrointestinal hemorrhage contributed to 3% of hospitalizations and 2.35% of in-hospital deaths among patients with hepatocellular carcinoma as a primary or secondary diagnosis, according to a Dexur analysis of 2013-2017 Medicare claims data.
The in-hospital mortality rate was 13% for GI hemorrhage with major complications (DRG 377) and 2% for GI hemorrhage with non-major complications (DRG 378).
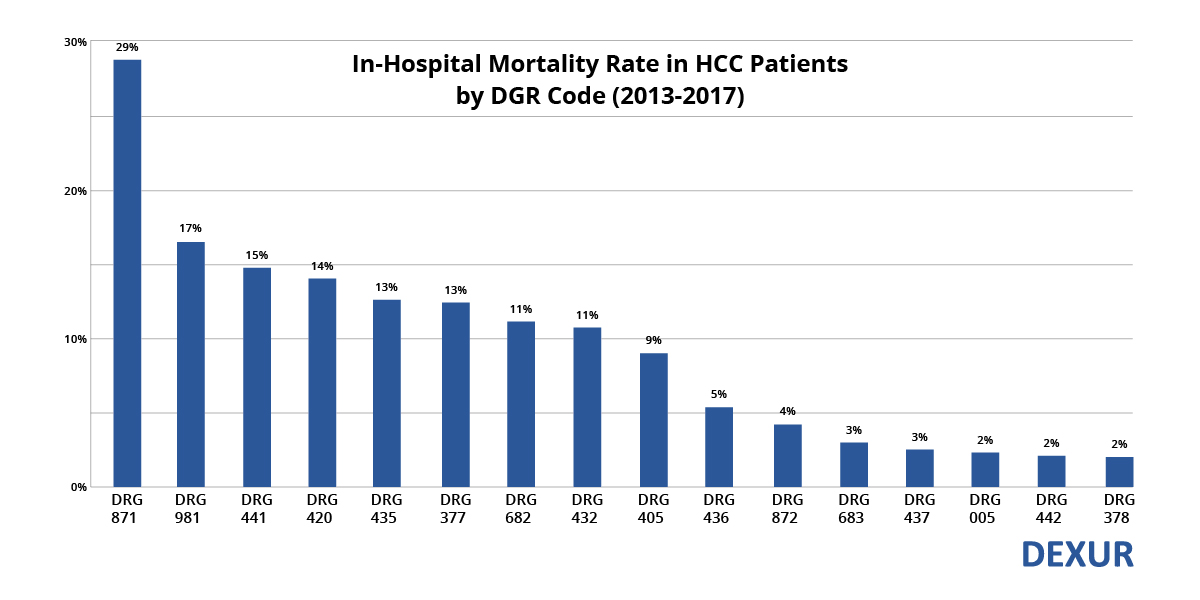
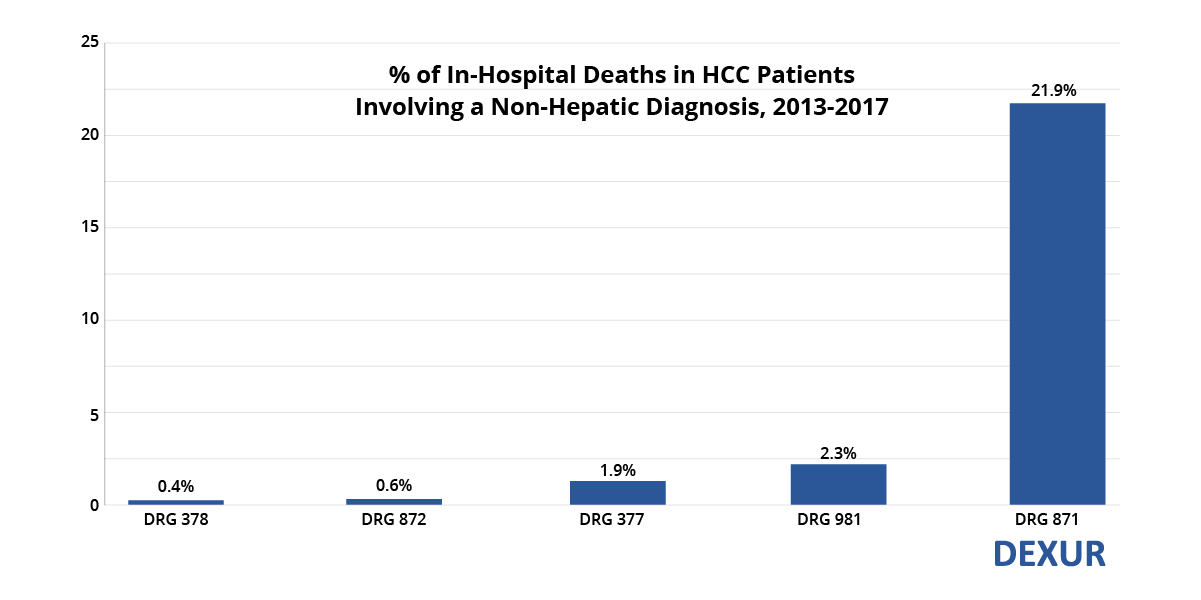
Sepsis was the most lethal comorbidity in HCC patients. 29% of HCC patients diagnosed with sepsis with major complications (DRG 871) expired in-hospital. As Dexur has previously reported, 22% of in-hospital deaths in HCC patients involved sepsis from 2013 to 2017. OR procedures unrelated to the primary diagnosis (DRG 981) also contributed to a noteworthy percentage of in-hospital deaths in HCC patients.
The literature contains many case reports on GI bleeding in hepatocellular carcinoma, but few systematic studies more recent than the 1990s.
Most case reports focus on HCC infiltration of the GI tract, including the stomach, gastric wall, colon, and duodenum. Chen et. al (1990)'s estimate that 2% of HCC patients experience GI hemorrhage is widely cited. However, most subsequent investigators reject Chen et. al's conclusion that direct tumor invasion of the GI tract is the most common cause of GI bleeding in HCC.
Yeo et. al (1995) conducted the largest prospective study of GI hemorrhage in HCC. Over 11 months, 55 patients with HCC presented with signs or symptoms of upper GI hemorrhage at the investigators' hospital in Hong Kong. Yeo et. al reported that the causes of the bleeds included 26 variceal bleeds, 15 peptic ulcers, and only 3 direct tumor invasions of the GI tract.
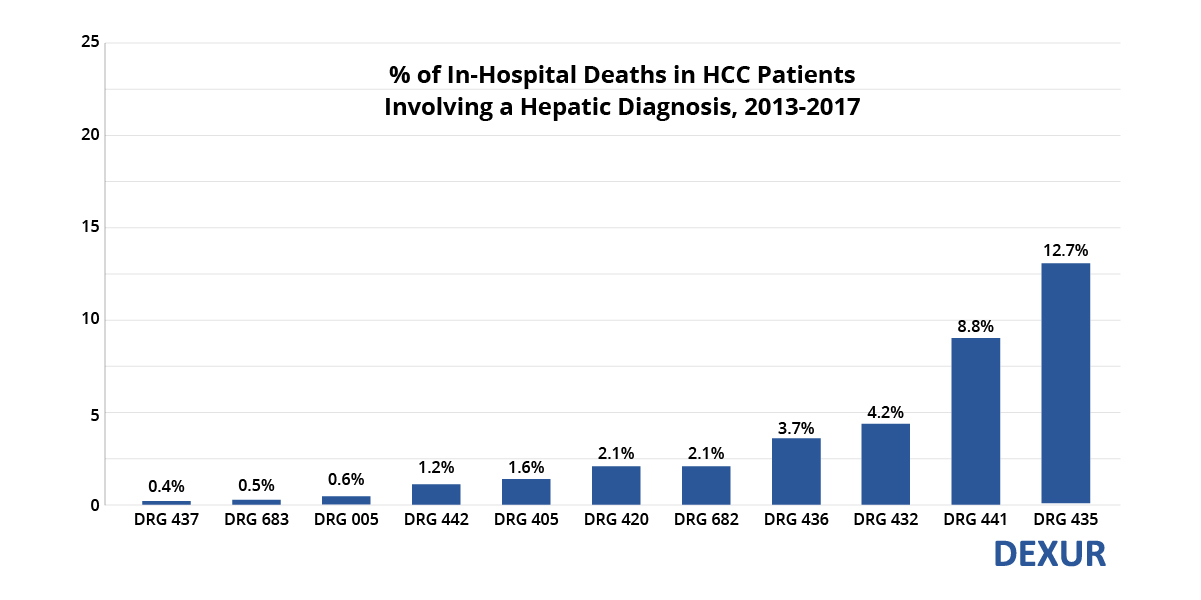
The most common causes of hospitalization and death in HCC patients are sepsis and complications of the underlying liver disease. However, GI hemorrhage is a significant contributor that physicians should be alert for.
ABOUT THE AUTHOR
