How to Evaluate the Impact of Venous Thromboembolism (VTE): Part 2: Incidence
In Venous Thromboembolism (VTE)
Get Dexur’s Personalized Hospital Specific Presentation on Quality, Safety, Compliance & Education
By: James Pitt Aug. 13, 2018
Hospitalized patients are at greater risk of venous thromboembolism than the general population, in part because immobility increases VTE risk. According to the CDC report on healthcare-associated VTE, up to 70% of HA-VTE cases are preventable.
Two measures of in-hospital VTE incidence can affect hospital reimbursement.
The first is AHRQ PSI-12, part of the PSI-90 composite. It reflects VTE rates in surgical patients.
The second is VTE-6, which reflects both prevention and actual incidence of VTE in patients overall.
VTE-6 is one of the six CMS Electronic Clinical Quality Measures that relate to preventing healthcare-associated VTE. Hospitals can report these as part of the Hospital Inpatient Quality Reporting program, which links in to CMS's value-based care initiatives. The other five measures only reflect preventative steps.
Some physicians have expressed concern that measuring VTE incidence will produce misleading results due to surveillance bias. Surveillance bias can make preventative measures paradoxically seem to increase the condition they are meant to prevent, because previously undetected cases are now detected. Dr. Karl Bilimoria and others at Northwestern University's Feinberg School of Medicine have published several studies on this topic, including a 2013 JAMA study in which they found that hospitals that performed more imaging and prophylaxis to detect and prevent VTE reported higher VTE incidence.
For this reason, Dexur recommends also using readmissions as a check.
As an example, analysts compared in-hospital rates of venous thromboembolism at six Pittsburgh hospitals.
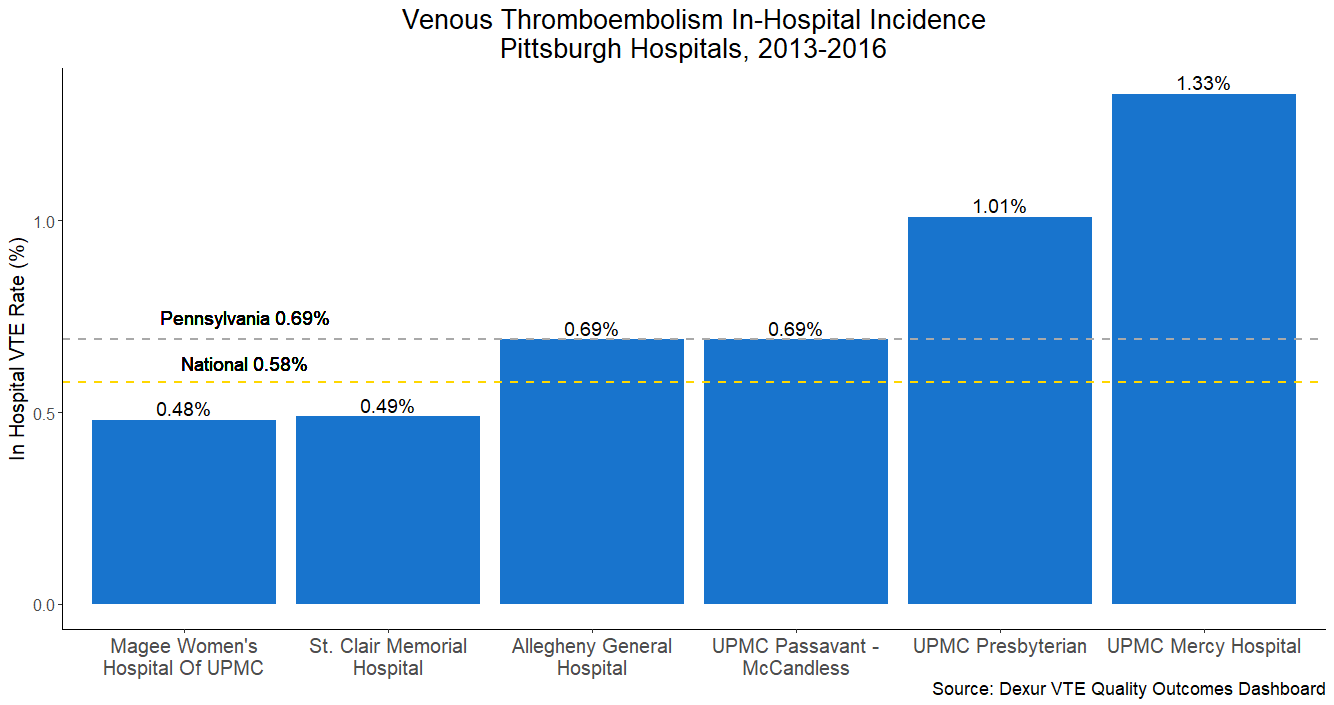
The highest incidence rate was 1.33% at UPMC Mercy Hospital, and the lowest 0.48% at Magee Women's Hospital of UPMC. Overall, these hospitals were close to Pennsylvania's state average VTE incidence.
DEXUR PRO MEMBERS GET ACCESS TO:
- Total All Inpatient Medicare Discharges
- In Hospital VTEs
- In Hospital VTE Rate (%)
- State In Hospital VTE Rate (%)
- National In Hospital VTE Rate (%)
- Excess Days over Avg. LOS
- Average Excess Days over Avg. LOS per VTE Discharge
- VTE Related LOS Outliers
- VTE Related LOS Outlier (%)
- State VTE Related LOS Outlier (%)
- National VTE Related LOS Outliers (%)
- Excess Days from VTE Related LOS Outliers
From 2013-2016, for CMS inpatient discharges at the following hospitals:
- UPMC Presbyterian (Pittsburgh, PA)
- Allegheny General Hospital (Pittsburgh, PA)
- UPMC Passavant - McCandless (Pittsburgh, PA)
- UPMC Mercy Hospital (Pittsburgh, PA)
- St Clair Memorial Hospital (Pittsburgh, PA)
- UPMC St Margaret (Pittsburgh, PA)
- Magee Women's Hospital of UPMC (Pittsburgh, PA)
ABOUT THE AUTHOR
